Dictionary.com provides a simple medical definition for addiction of “Habitual psychological and physiological dependence on a substance or practice beyond one’s voluntary control”. Additionally, two scientific definitions of addiction are given as (1) “A physical or psychological need for a habit-forming substance, such as a drug or alcohol. In physical addiction, the body adapts to the substance being used and gradually requires increased amounts to reproduce the effects originally produced by smaller doses” and (2) a “habitual or compulsive involvement in an activity such as gambling.”
So What Are We Dealing With?
It’s not particularly helpful or accurate to conceive the nature of addictions as twofold: either involving habitual activity (like gambling or shoplifting), or involving substance abuse (such as prescription or recreational drugs, alcohol). If we just scratch the surface of one addiction both physical and emotional factors are swiftly revealed. Smoking, for example, carries an element of ritual in the habit (the lighting up, sharing with a friend, the last course of a satisfying meal and so on)as well as a degree of physical or cellular dependence on nicotine and likely damage to the respiratory system. The case is similarly so with recreational or even prescription drug abuse, where it can be the obtaining of an illegal substance (scoring) and the sociability or excitement that can be involved, or with a quick visit to the pharmacy to redeem your prescription or pick up a quick packet of paracetamol for those odd aches and pains. Physical repercussions in these examples can result in respiratory or digestive compromise.
Habitual or ritualistic conditions such as trichotillomania (pulling out one’s own hair) or shoplifting (kleptomania) can also result in physical repercussions: damage to the hair follicle and growth cycle in this first instance and possibly adrenal overload in the second, so consideration of, treatment or cure for any type of addiction has to involve a fair degree of physical and emotional unpicking as well prioritising the significance of each aspect of the addiction to the habituée. Once these issues have been untangled, treatment can commence.
Another important aspect to consider is the difference between addiction and abuse, because it is possible to abuse a substance or overdo a habit without being clinically or physically addicted to it. According to https://addictionresource.com/addiction/, abuse involves certain criteria such as failing to fulfil responsibilities because of using a certain substance, continued usage despite full knowledge of the damage it causes, legal problems arising from its use and reckless behaviour whilst on it or trying to obtain it.
Addiction, on the other hand, is considered to be a more serious issue than abuse, because the person cannot physically stop: at this point of the process, the brain has actually been altered to crave the substance in question in order to function normally. Importantly, all pleasures are registered by the brain in the same way, regardless of whether the pleasure originates from a psychoactive drug, satisfying behaviour, sex, or a delicious meal.
Brain imagery reveals that drugs and other substances become addictive because they don’t just alter the neurons in the brain, they also biochemically change behavioural patterns. This is because the neurotransmitters in question (dopamine and glutamate) are located in not only the brain’s pleasure centre (the Nucleus accumbens) but also in the area concerned with judgment and decision-making (the Amygdala), as well as memory (Hippocampus). Fig 1 below illustrates.
As tolerance (as it is commonly named) builds up to the habit involved, increasing amounts of the substance or more frequent behaviours are required by the person involved in order to feel their original gratification, so consequently the brain now perceives the drug or activity itself as being the source of pleasure. Then the person behaves increasingly recklessly in order to obtain their satisfaction.
A shortcut to the brain’s reward system has been set up by the dopamine flood, which reacts with the glutamate in the hippocampus and in the amygdala to entrench memories of this rapid sense of satisfaction. A conditioned (or learnt) behavioural response is thus established and the end result is that addictive substances and behaviours firstly stimulate this reward-related learning circuit and then overload it.
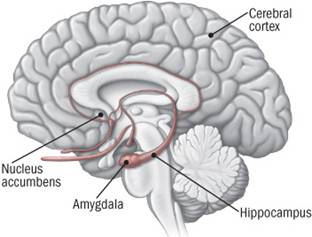
Fig 1: The Brain’s Pleasure Centre / Reward Circuit
Additionally, the likelihood of both drug usage and any rewarding activity resulting in addiction is directly linked to the speed of this dopamine surge – and also to the intensity and reliability of its release. Taking the same drug via different methods also influences the likelihood of addiction, so smoking a drug or injecting, as opposed to swallowing it will produce a more robust dopamine signal and hence is more likely to result in misuse. The resource http://www.helpguide.org/harvard/how-addiction-hijacks-the-brain.htm clarifies.
After ‘tolerance’ is reached (when the dopamine has less impact on the brain’s disrupted reward centre), what is termed ‘compulsion’ takes over. DP’s Case Outline 1 below illustrates the tolerance stage. At the compulsion stage, the pleasure associated with the habit has subsided, but the memory of the desired effect and associated need to recreate it persist. The associated environmental cues and information set up in the reward circuit as memories have helped to create another conditioned response – that of intense craving or compulsion – whenever the person encounters them. I thought that JR in Case Outline 2 had reached this point when she first sought my help.
It is also held that the cravings and conditioned learning explain not only the addiction itself but also any ‘relapses’ after periods of ‘remission’ or abstinence before ‘recovery’ is achieved (Kendall & Hammen 1998). For example, someone addicted to heroin may be in danger of relapse on seeing a hypodermic needle, whilst another may be start drinking again after being near a bottle of vodka. Abstinence periods may often be quite lengthy and the person will no doubt need extra support and encouragement should they relapse and feel tempted to indulge again (see below).
Whilst we have a few things explained in somewhat Pavlovian terms, what else can we do as homeopaths about the remainder of the addiction tapestry and the most important threads of the story? Where do we start? What do we take into account and prioritise? Should the questions of when substance usage or habitual behaviour become pathological – and to whom – be included?
Starting the Journey
There is one key consideration for both patient and practitioner at the outset of treatment and that is simply a question of establishing whether or not the person is actually ready and motivated to kick their habit and commit to a curative process. The fact that someone has sought help in the first place is an encouragement but unless there is evident personal commitment that both patient and practitioner can clearly pin down, the journey to cure will be a fruitless one.
CBT-type strategies such as identifying any thoughts that trigger the habit, separating the resulting emotion from each thought and then pinning down the behaviours that are driven by these (Foreman & Pollard 2011) may be helpful to both homeopath and patient. In other words, it may help to be clear about how thoughts (which are not facts)affectthe way the patient feels (about the habit and themselves) and then behaves as a consequence.
Should the habituée hold any negative thoughts around the ability to change old habits and create new ones or about change itself, then time needs to be spent around exploring what beliefs and assumptions support this hindrance. Negative thinking often appears automatically and unbidden – particularly in those with low self-esteem –but once these automatic negativities are identified, they can be balanced and replaced by positive, alternative thinking (Foreman & Pollard 2011). Writing things down in a format like Table 1 below gives an example of how this can be done in the context of someone trying to give up smoking.
A simple pros-and-cons exercise like Table 2can also be used to help weigh things up. Again, I’ve used the context of giving up smoking, or a nicotine addiction to illustrate this. (Of course, the tables need not be actually used, they are merely suggested as a possible framework. Not everyone finds it constructive or necessary to write things down).
Additionally, the likelihood of both drug usage and any rewarding activity resulting in addiction is directly linked to the speed of this dopamine surge – and also to the intensity and reliability of its release. Taking the same drug via different methods also influences the likelihood of addiction, so smoking a drug or injecting, as opposed to swallowing it will produce a more robust dopamine signal and hence is more likely to result in misuse. The resource http://www.helpguide.org/harvard/how-addiction-hijacks-the-brain.htm clarifies.
After ‘tolerance’ is reached(when the dopamine has less impact on the brain’s disrupted reward centre), what is termed ‘compulsion’ takes over. DP’s Case Outline 1 below illustrates the tolerance stage. At the compulsion stage, the pleasure associated with the habit has subsided, but the memory of the desired effect and associated need to recreate it persist. The associated environmental cues and information set up in the reward circuit as memories have helped to create another conditioned response – that of intense craving or compulsion – whenever the person encounters them. I thought that JR in Case Outline 2 had reached this point when she first sought my help.
It is also held that the cravings and conditioned learning explain not only the addiction itself but also any ‘relapses’ after periods of ‘remission’ or abstinence before ‘recovery’ is achieved (Kendall &Hammen 1998). For example, someone addicted to heroin may be in danger of relapse on seeing a hypodermic needle, whilst another may be start drinking again after being near a bottle of vodka. Abstinence periods may often be quite lengthy and the person will no doubt need extra support and encouragement should they relapse and feel tempted to indulge again (see below).
Whilst we have a few things explained in some what Pavlovian terms, what else can we do as homeopaths about the remainder of the addiction tapestry and the most important threads of the story? Where do we start? What do we take into account and prioritise? Should the questions of when substance usage or habitual behaviour become pathological – and to whom – be included?
Starting the Journey
There is one key consideration for both patient and practitioner at the outset of treatment and that is simply a question of establishing whether or not the person is actually ready and motivated to kick their habit and commit to a curative process. The fact that someone has sought help in the first place is an encouragement but unless there is evident personal commitment that both patient and practitioner can clearly pin down, the journey to cure will be a fruitless one.
CBT-type strategies such as identifying any thoughts that trigger the habit, separating the resulting emotion from each thought and then pinning down the behaviours that are driven by these (Foreman & Pollard 2011) may be helpful to both homeopath and patient. In other words,it may help to be clear about how thoughts (which are not facts)affectthe way the patient feels (about the habit and themselves) and then behaves as a consequence.
Should the habituée hold any negative thoughts around the ability to change old habits and create new ones or about change itself, then time needs to be spent around exploring what beliefs and assumptions support this hindrance. Negative thinking often appears automatically and unbidden – particularly in those with low self-esteem –but once these automatic negativities are identified, they can be balanced and replaced by positive, alternative thinking (Foreman & Pollard 2011).Writing things down in a format like Table 1 below gives an example of how this can be done in the context of someone trying to give up smoking.
A simple pros-and-cons exercise like Table 2can also be used tohelp weigh things up. Again, I’ve used the context of giving up smoking, or a nicotine addiction to illustrate this. (Of course, the tables need not be actually used, they are merely suggested as a possible framework. Not everyone finds it constructive or necessary to write things down).
Table (1): Negative Automatic Thinking Example
| TRIGGER | AUTOMATIC THOUGHT | NEW RATIONAL THOUGHT |
| A challenging day at work | “I just can’t wind down so I’ll have another cigarette to relax” | “I’m taking a while to wind down so I’ll go swimming after work” |
Adapted from author’s notes (2013)
Table (2): Pros & Cons of Giving Up Smoking
| Benefits (pros) | Costs (cons) | |
| CHANGING | ~ Less breathlessness & improved health
~ Able to exercise more to relax ~Will save money & won’t smell of smoke ~ Partner/children really want me to stop |
~ Coping with cravings
~ Missing the social side ~ Might get more stressed – it’s relaxing for me ~ It’s very hard for me to change |
| STAYING THE SAME | ~ Don’t have to go through all the effort and will power needed to give up
~ It’s easier for me |
~ Health will get worse
~ Will still be short of money ~ Will still have hassles with partner over finances/health ~ Passive smoking bad for kids& partner’s health ~ Children might copy me & think It’s OK to smoke |
Adapted from Foreman & Pollard (2011)
As mentioned earlier, the fact that the person has come to you for help is an optimistic and constructive start. If it can be established that there is a value or purpose attached to the habit in question, itcan be useful to illuminate circumstances at the onset of the problem, assess its current impact upon the individual and/or gauge the degree of actual pathology involved.Relevant remedies would also assist clear and objective thinking for the patient.
As described earlier, should a relapse occur somewhere down the line, CBT techniques like balancing negative thoughts (eg self-depreciation) with positive, constructive alternatives, alongside with appropriate remedies, could beusedagain to re-cement cracks in the healing pathway.
But now to return to the beginning and the more homeo-therapeutic realms.
Therapeutic Choices
Organotherapy of some kind is part of most holistic approaches to addiction. Organ or system supportand/or drainage or detoxification is nearly always appropriate alongside remedies focussedmore upon emotional priorities.The damage done to the body by over-use of various addictive substances are widely documented, and there are several options available for homeopathy to help the body recover, detox if necessary and to re- regulate functionality.Practitioners usually have their own preferences with this, but here are some choices:
Sarcodes are of immense value to encourage compromised organs to return to a healthy level of functioning and these remedies can be used alone or in combination with affiliated remedies and herbs. I usually select a low C potency.
Tinctures can be used as therapeutic combinations, either in herbal form or as a mother tincture. Their equivalents in homeopathic potency (ideally a low X) can also be of great help, for some patientscan dislike taking tinctures or capsules or may wish to avoid alcohol completely. Also, and increasingly so these days,a particular herb may become unavailable or difficult to source so it is reassuring that the energetic form of most herbs can be represented homeopathically.
Tissue Salts provide another straightforward option for cellular level assistance. Some practitioners may not feel particularly confident or comfortable about using sarcodes or herbs and if so, can fall back reliably on Schuessler’ssupport method.
Tautopathics
Addictions present us with another effective and helpful prescribing are na: that of tautopathy, which I see as the perfect mirror for ‘what will cause will cure’ – the cause of physical discomfort is obvious and specific and the aetiology is direct. Ian Watson (1999) reports “As long as the nature of the substance is known, it can be potentised and given back to the patient like any other remedy”. He goes on to say that there is plenty of empirical evidence that tautopathy eases the withdrawal of drugs and medications. This is because the potentised form of a drug enhances its elimination in order to make it a less traumatic process for the body, but essentially of course, withdrawal has to be done gradually.
As we’ve seen above, the goings-on in the brain’s pleasure centre to reach the ‘tolerance’ and ‘compulsion’ stages along the road to addiction and mis-use mean that the condition can have a tenacious hold upon both mind and body. It is a grip that needs to be released in a gentle fashion rather than going ‘cold turkey’ as is so often portrayed in films. It is also something to be impressed on the patient should they tend to be on the all-or-nothing (sycotic!) side.
Miasmatics
Undoubtedly, a miasm or two will be lurking in the background and/or presenting in the foreground. I’ve found that those at work are more likely to be the sycotic or the syphilitic miasmor bothin patients with addictions, but of course this would not necessarily be the case with everyone. Consider a hoarding habit for example, where apsoric picture could well be significant. Here, the patient’s motivation behind the habit and the value they attach to it would be the maindeterminants: an Arsenicum would hoard for a different purpose than a Psorinum or a Medorrhinum.
Medorrhinum-Americana is typically a syco-syphilitic remedy, whereas Medorrhinum is predominantly sycotic. Colin Griffith (2015) ascribes nature of the former to its source: “degenerative processes arising from an addictive personality – very similar to Medorrhinum but more syphilitic and therefore destructive”. This also reminds me of the importance of the patient’s inherited family health patterns when treating addictions because behavioural patterns as well as dis-ease traits and traumacan be passed down in our miasmatic luggage. Perhaps this alsobacks up the notion that there is an ‘addictive personality’.
It is generally accepted in homeopathy that recreational drugsand heavy drinking can awaken a dormant miasm, but a consideration of which miasmatic influences are at play and to what extent, coupled with checking indicated remedy affiliations (to evident miasms and especially the most dominant) can also help with differentiating and choosing support remedies.
Timeline
A detailed and rigorous timeline is an asset to any case, but with treating addictions, it is particularly useful for identifying aetiologies as well as deciding where and when to make relevant remedial interventions.For example, withDP the aetiologies were clear but there was no need for digestive support because his distressing symptoms were directly relieved by cutting down and stopping the Neurofen Plus. His RSI symptoms had begun prior to the addiction and were basically a maintaining cause. It is also possible that his former attention to diet and exercise, albeit somewhat obsessive, had stood him in good stead. In JR’s case, physical support was immediately called for alongside major remedies and the overall improvement to her hair quality also provided extra encouragement for her to stop her habit.
The Constitutional
I have found that a constitutional or totality remedy is invariably called for, but not necessarily at the outset. I usually give this as a consolidation for cure for the addiction and resolution of its underlying issues, rather than at the beginning of the journey or as a choice of methodology. This is simply because there is an obvious overlay to a previous and healthier state before the addiction developed; and of course,we are dealing with what is ‘on top’ for the patient.
Ending the Journey
Addictions, needs or compulsions are of many different manifestations and origins according to each individual’s expression of them. Understanding the complex nature of problems like these and what each aspect represents to the person involved is therefore central to providing appropriate treatment on several levels of health. Informed homeopathy can provide an ideal and significant way forward in helping people relinquish unhelpful and harmful habits and regain their physical and emotional well-being.
| CASE OUTLINE 1
DP (aged 38) became addicted to Neurofen Plus. He started to take them to relieve his RSI symptoms that had not responded to paracetamol, ibruprofen or aspirin and because his GP was “unhelpful”. He had also recently split up with his wife of 10 years and been sacked from his job. DP quickly went onto double the recommended dose of the drug, despite clear warnings on the product Information sheet that Neurofen Plus is a short-term medicine only with a maximum recommended dose of 6 in 24 hours and that its active ingredients are addictive, causing withdrawal symptoms. These matched those he was experiencing, along with those relating to the RSI. DP also had a history of recreational drug taking and heavy drinking as a younger man which was replaced in more recent years by a high protein diet, going to the gym and running “all to excess”. He had always been a loner and an outsider since school years, confiding only in his sister (6 years younger) who had a history of anorexia and addiction to exercise in the past. Physical Symptoms: Insomnia, twitching, aching fingers, stiff wrists, muscle spasms, digestive disruption, “unsure if awake or dreaming”, when does sleep dreams are “crazy & tortured”. All sxs>>hot baths, fresh air; << sun, <<“suspicion”. Emotional Picture: DP didn’t associate any particular value or purpose to his over-usage – just the compelling physical need to “take it in stronger doses to be reasonably ok”. But he also recognised and acknowledged that he had to stop in order to regain some structure and self-respect in his life. Motivations for Stopping: Ashamed of self. Stopping meant access to his sons aged 6 & 3 and the ability to commit to regular work again. Prescription 1: Arnica/Act-Spic/Ruta 200C combination daily/as required; Med LM1 water dose daily, Nurofen Plus 12C t.d.s./p.r.n. to replace the drug on alternate doses and then on alternate days in order to withdraw them slowly. Intent: Symptomaticrelief of RSI symptoms; active miasm; tautopathicsupport. Outcome: DP gradually reduced the frequency of all homeopathic remedies as his withdrawal progressed & all physical symptoms were reduced as a result of both the RSI remedies and the tautopathy. With the Med LM1 daily, DP found it “surprisingly easy to get a grip again” and there was no need to changeany potencies. An underlying Pulsatilla totality was revealed which I had intended to give as a constitutional after about 3 months. Within10 weeks DP had found another job in a coffee outlet with opportunities to progress, had regular access to his sons again and had regained much of his self- respect. I didn’t get the opportunity to give Pulsatilla… |
| CASE OUTLINE 2
JR came to me because she compulsively pulled out her own hair from the back of her scalp on the crown whenever she was stressed. Sometimes she did this unconsciously or had not remembered she had done so. Triggers were always work or performance-related and rooted in her self- perception of not being good enough. JR had pulled her hair earlier in life at stressful times, starting at aged 14/15 at exam times and when starting work for the first time. She is now aged 49. We identified that the original and underlying trigger was the need to be liked and to gain approval from others which in turn stemmed from being bullied at school. (Interestingly, JR did not feel the inclination to pull in the most traumatic times in her life – her father’s death, mother’s dementia diagnosis and own previous cancer scare). Feels more confident about voicing concern over her habit but needs to stop and doesn’t know how. Symptoms: Sometimes prompted by twiddling or stroking her hair, JR feels differences in root and texture, pulls out the most different, examines it, discards and then must find more similar hairswhich are also discarded. She gains a feeling of “peace and achievement”, appreciates “the cold feeling” then becomes upset because it’s a bald patch, which provokes further “panic” because of what others will think. Hastried pulling from other areas of scalp but this area feels “positive” to her. If pulled patch is small, must make it bigger.>occupied with something specific, > shouting, > going to gym. Motivations for Stopping: Concern over re-growth of hair and others’ opinions of her. Prescription 1: Kali-S6X/Nat-M6X/Sil12X tissue salt combination; Syph LM1 &Aur LM1 water doses on alternate days. Patting self on the back when achieving& choosing a diversion activity at first signs of inclination to pull hair. Intent: Support for hair growth cycle. Very active miasm. Self-sabotage & not being good enough are twin issues of equal significance. Symbolic yet powerful recognition/reinforcement of personal achievement. Outcome: JR only felt a need to pull 2-3 times in 3 weeks and diverted herself with colouring books and by shouting out loud (in private). She negotiated a work-from-home option 1 day per week and felt encouraged by her new hair growth/renewal as well as its improved texture. Prescription 2: Repeat with option to alternate Syph and Aur weekly if feels need. Intent: Ongoing cellular support for hair and gentle, all-round benefit from both remedies. JR recognised how the remedies had begun to resonate with her and how she would know when she no longer needed them. Outcome: Within 4 months of treatment JR felt that both AurLM1 and the tissue salts had completed their work for her and was taking Syph LM1 on a weekly basis. She no longer felt the urge to pull her hair at more stressful times and her emotional picture was generally very positive. JR still felt the need for a weekly “pick-me-up” for the moment. 8 months on, she is confident and at ease with herself. I have prescribed her constitutional remedy Calc-Carb to consolidate her overall cure. She “checks-in” with me on a seasonal/p.r.n. basis. |
BIBLIOGRAPHY/REFERENCES:
Griffith, Colin (2015): The Comprehensive Repertory of New Homeopathic Remedies: A Guide to Strategic Prescribing, Watkins
Foreman, Elaine & Pollard Clair (2011): Introducing CBT (Cognitive Behavioural Therapy): A Practical Guide, Totem Books
https://addictionresource.com/ [accessed 14 Sept 2016]
http://www.dictionary.com/browse/addiction?s=t [accessed 12 Sept 2016]
http://www.helpguide.org/harvard/how-addiction-hijacks-the-brain.htm [accessed 19 Oct 2016]
Kendall, P C &Hammen C (1998): Abnormal Psychology: Understanding Human Problems, 2nd edition, Houghton Mifflin Company, Boston, New York
Reckitt Benckiser Healthcare International Ltd, Nurofen Plus Product Information Sheet, April 2012 revision
Watson Ian (1999): A Guide to the Methodologies of Homœopathy – Cutting Edge Publications, Kendal, Cumbria, England, Revised edition the need or strong desire to do or to have something, or a very strong liking for something.


