Abstract
Homeopathic treatment of a young male child over the course of 2.5 years resulted in the amelioration of periodic limb movement disorder and restless legs together with improvement in accompanying behavioural issues. Through individualisation, a decrease in occurrence and change in the nature of acute illness, simultaneous to the improvement of the chronic issues, were witnessed.
This case progressed congruent to the hierarchy within the three levels of the human being, once the correct remedy was established. This positive progression signified an increase in the Level of Health of the patient. By prescribing the simillimum and exercising restraint with dosing, long term amelioration was observed. However, to achieve this, the case needed to be monitored closely and followed up regularly.
Keywords homeopathy, individualised treatment, restless leg syndrome, period limb movement disorder, children, behavioural problems, acute illness, levels of health
Introduction
Two important pillars of classical homeopathy are the Law of Similars and the Law of Minimum Dose, and the following case study will show these two important homeopathic laws in action. Individualisation, the cornerstone of the homeopathic treatment, will also be illustrated here in terms of the remedy selected, as well as the potency and repetition of dose.
In homeopathic prescribing, when the simillimum is given, the patient often undergoes healing as a process, as the body finds its way towards homeostasis. If an issue is longstanding, this may take time and go through different spheres as the treatment progresses.
The direction of cure, also central to homeopathic theory and the analysis of remedy reactions, is based on the hierarchy within the three levels of a human being – mental, emotional, and physical, respectively. Within each sphere is yet another hierarchy; for example, the physical plane is divided into the functional body systems of which the most vital organs (brain and heart) to the least vital (bone and skin) form part.
During correct homeopathic treatment, the disturbance can go from the mental to the emotional or to the physical plane, or the issue may stay on the physical but move through different types of chronic physical ailments.
Acute physical illnesses can also change in nature; for example, may affect a person more superficially, and can reduce in severity and frequency. These can all be indications that a person is becoming healthier and more resilient and increasing their Level of Health.1
Homeopathy has been widely used to treat behavioural problems in children, due to its effectiveness and ease of administration.2,3 Many over-the-counter remedies have been touted as being able to “calm children”;4 however, to prescribe most effectively in chronic cases classical homeopaths treat the child as a whole, without assuming a “this is for that” approach.
If a remedy is given when it is not indicated, there can be a variety of outcomes. This case study further demonstrates how a partially acting homeopathic remedy (close, but not the simillimum) can alleviate an important physical symptom without improving the emotional and mental symptoms: As per the direction of cure and the abovementioned hierarchy, this is not a good outcome and indicates the remedy is not correct. Thus, this paper may serve as a reminder that homeopathy is about treating the entire person, not just their isolated symptoms.
Case report as per initial consultation
Nature of the complaints
A 6-year-old child presented with behavioural problems and extreme restlessness. The behaviours first became apparent when he began school two years earlier. His behaviour is worse when away from his mother and when forced to sit still. The behavioural issues are constant, and underlying them are anxiety, mostly separation anxiety, and a sensitive constitution.
His legs are extremely restless, and he cannot keep them still, and this symptom is very much long term. When he was an infant, he had a sleep study done – the results showed that he woke a substantial 16 times an hour and was diagnosed with periodic limb movement disorder. Movement ameliorates, and he is worse when he lies down to go to sleep. The restlessness, and wriggling of his legs, is constant. He describes the sensation as “my legs are stretchy”.
The child has sensitivity to noise. He feels the need to talk loudly over noise e.g., in a restaurant he will exclaim “these people are so loud”. He does not like it if there is too much noise going on. He has an obsession about insects. He “loves bugs” above all else.
He complains of itchy and sore eyes, mostly the left but can be the right too. At times he grinds his teeth. He has trouble pulling his foreskin back – he does not say it hurts, but when he urinates, it balloons. Last year he had balanitis, aggravated by washing the penis with soap, which required antibiotic treatment. He is always holding his penis and can be seen doing it in every photo that is taken of him. He does not hold it because he needs to urinate, he is “just holding it”.
The child is hotblooded, never wants to be tucked in at night, and finds his way out of the bedding. He drinks cold water and does not like anything warm or hot. The child eats mostly a raw diet and when he eats cooked food, he gets thirsty.
He craves salty and fatty foods e.g., macadamia nuts, coconut. Seeds and nuts give him a sore stomach. He will ask for sweets such as ice-cream, but he won’t eat it – he says it’s too sweet. He will eat dates. He does not like refined sugar. His mother suspects multiple allergies.
He wakes early, always, at 5am, and won’t go back to sleep. This used to be because of urging for stool. His mother has intensively endeavoured to heal his gut, so the need for stool is no longer the reason he wakes. She wakes the child at 10pm to take him to the toilet, but he still wakes at 5am to urinate. Sometimes he will wake up suddenly and yell for his mother but will go straight back to sleep.
He escapes the classroom, but not from home. He does not want his mother to leave him at school. His restlessness at school manifests as such: he won’t stay still, during nap time he has an aversion to going to sleep, he must keep busy, and he hadn’t been sitting still at story time.
He was interrupting, so the teacher gave him things to do with his hands – then he sat and listened to the story. The school has needed to have a full-time teacher aide on site specifically to physically restrain him during story time/assemblies and to chase after him when he escapes. Other parents had complained the child was disrupting the learning of the other students.
According to his mother, he doesn’t seem to think: There is no thought process. He is not considerate, only thinks about himself or insects, he doesn’t think about people. He will ask for inappropriate things at inappropriate times. The mother says this is non-stop e.g., she will tell him she’s busy, but he doesn’t get it. He wants her to watch him, to see what he’s doing. She says he is selfish and “he could be Asperger’s”, though no diagnosis has been sought.
Personal medical and family history
Two weeks over his due date, the child was born via caesarean section. He suffered from tongue tie, lip tie, had difficulty breastfeeding, had two rounds of antibiotics through breastmilk within about three weeks of birth (mastitis), and suffered from terrible reflux, sleeping issues and colic.
He was put on a particular formula (intended to stop reflux, something that hardens in the stomach and turns milk solid) which meant his stools were like rocks. He had general anaesthetic at approximately 22 months old to rectify the tongue and lip ties.
At 17 months old, he suffered from pneumonia and Respiratory Syncytial Virus (RSV) simultaneously and was hospitalised for about a week and treated with IV anti-biotics and oxygen. He has had many colds and flues and a couple of gastrointestinal viruses. The child is prone to intestinal worms. He has not had any vaccinations
He had positional talipes where the feet turn in (like club foot) when he was born. The mother believed it was from the position he was lying in the womb: being 2 weeks overdue and being a “giant baby”, he was “squished up” and his feet had turned inwards. The parents had to do exercises on his feet and massage them. The mother wonders if the current feeling of stretchy legs has something to do with this.
The child’s maternal grandmother has severe restless leg syndrome and is medicated for it, so there is the possibility of a genetic predisposition. She also has Hashimoto’s thyroiditis and fibromyalgia. Scoliosis is an issue for both his mother and maternal grandmother. There are also stroke and heart complaints on the mother’s side, as well as brittle bones. The child’s maternal grandfather gets reflux and sleep apnoea.
The paternal grandmother had parathyroid issues: high calcium levels, and a tumour on the parathyroid gland, which had to be removed. She has poor vision that required laser surgery. The patient’s father also has vision problems, has a tendency towards depression and alcoholism, and smokes tobacco.
When I asked about the patient’s eyesight it was apparent that he did not have any issues with his vision as his ability to spot tiny insects is phenomenal – one of the school staff saw him running across the lawn, stopping suddenly before doing a complete U-turn because he had spotted an ant amongst the blades of grass!
Homeopathic perspective and intervention
The depth of the disturbance from a homeopathic point of view is relatively superficial – he is not a deeply disturbed individual, although he is sensitive, and the disturbance has been there since he was a very young infant. The anatomopathological disturbance is upon the nervous system and affects the limbs.
The immune system is also likely disturbed (allergies) as well as the respiratory system, and the nature and the frequency of the acute infections place the child as a Level 5 in Group B according to the Levels of Health theory.5
No psychological diagnosis has been sought, despite the mother’s concerns. I can see from the case-taking that, like in autism spectrum disorder, there is a restrictive range of interests and lack of understanding and reciprocity in communication.
He also seems impulsive, and like in attention deficit hyperactivity disorder, he does not stop and think before talking.Individualisation is the cornerstone of homeopathic treatment. Therefore, differentiation of the remedies is paramount. The repertorization began as such:
Repertorization 1.
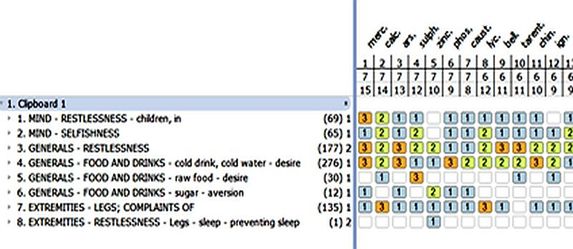
Since the extreme restlessness became the most important and intense symptom of the case, the main remedies I considered were Rhus Toxicodendron, Zincum and Tarentula. I also considered Asarum because of the noise sensitivity, a symptom I later added to the repertorisation. The issues with his legs and the “stretchy feeling” seemed like an indicator for Zincum. In the rubric EXTREMITIES – RESTLESSNESS – Legs – sleep – preventing sleep, Zincum is the only remedy listed there.
The mother explained to me that when the patient was younger, he was diagnosed with copper toxicity and was supplemented with zinc. Initially, taking the zinc supplement made him worse – more emotional, more anxious (she said this was to be expected due to a copper detox) but then he eventually became much calmer. The mother did not continue long term with the supplement.
I prescribed Zincum 30c on the spot. However, when I studied the case further, I realised that Tarentula was likely the better choice and I needed to ask more questions around this remedy.
Case report as per follow ups (over 2.5 years)
| DATE | FOLLOW UP | PRESCRIPTION |
| 1 week after three doses of Zincum 30c | The patient stopped complaining of “stretchy legs”, but the rest of the symptoms were not helped. It was not a good sign that the physical symptom of the leg discomfort improved while the emotional and mental symptoms were left untouched: Zincum was partially acting and not the simillimum.
The patient had an amelioration from music, he was obsessed with musical instruments”. She said that playing musical instruments was the only thing he ever does at home: “if he’s not doing bugs, he’s playing music”. She said he also loves to dance. He hits himself in the head and the sensation in his eyes is sandy, splintery, itchy. |
Tarentula 200C – one dose
(See repertorization 2.) |
| After 1 week | Despite instructions to only give it once the mother gave the remedy once in the afternoon and then re-dosed in the evening.
The next day he complained of a left sore upper arm/shoulder, and whined about his arm. He had a “fantastic day at school” (an amelioration of the behaviour with an aggravation on the physical plane is a positive reaction according to the hierarchy within the three levels of the human being). After 6 days he was a lot more cooperative. He slept until 6:30am (instead of the usual 5am wake up). He had become calm, and less agitated. The mother said that before the remedy it was almost like he wasn’t comfortable with his body, and that everything was annoying him. Now he seemed “more settled in his skin”. He still had “stretchy legs”, but the mother said there had been a definite emotional and energetic shift. She even felt different… She had become calm, and their relationship was better. They had become more understanding of each other. She said he had been “amazing at school”. His teachers had been really pleased with him. |
Wait |
| After 2 weeks | The child had said his legs felt so stretchy he needed to “shed his skin” and he started to relapse.
There had been glimpses of what he was like before the remedy, but he was still much better overall. There were short bursts of him before the remedy, but he improved on his own without the remedy being repeated. He sat on the teacher’s lap during a whole performance at assembly and did not run amok – he did as he was supposed to, but he wouldn’t have sat still without the teacher holding him. Apart from the shedding of the skin expression he hadn’t complained about his legs as much. After his usual bedtime leg massage, he wouldn’t wriggle his legs around as he used to, they were less restless, and they seemed to be more relaxed. The child’s mother said he is a perfectionist. He said he wished he was dead so he wouldn’t be able to do it wrong. As soon as he got home, he picked up his flute and sat outside and started playing it. The last week he had been playing music again, whereas he had not done so since the initial dose of the remedy. |
Tarentula 200c was repeated |
| After 2 weeks | The patient began having difficult behaviours at school again. The mother did not think he was having a full relapse because she put it down to it being the last week of a 10-week term and she observed that many of the other children were struggling at that time as well. The child was still relatively calm, more engaging and gave more eye contact than before the remedy. The mother said that for five days he had not complained of “stretchy legs” once, and she was very much astounded by this as it was the first time in his life that he had abstained from saying this for such a period of time.
When the school holidays were halfway through, and the mother told me that he had started having symptoms of rhinitis/hay fever. This was a new symptom, and a good direction of cure, from the lower respiratory tract to the upper respiratory tract. |
Wait |
| 3 months after the initial consultation | The mother was having to sit in class with the child during the morning session in order for him to stay in his seat and do his schoolwork. The child was not engaging with the teacher and with others – he had not been holding eye contact. The morning of the consultation the patient had told his mother that he “sees noise”. E.g., he had made a musical instrument out of toilet rolls, and he told her he can see the noise, not just hear it. The mother thinks this is why he struggles in the classroom, because of auditory/sensory issues. | The remedy was repeated, with the potency raised slightly – Tarentula 201C |
| After 4 weeks | The patient was much more engaging and made eye-contact readily as opposed to other times where he would not look me in the eyes.
The mother’s housemate had said “Wow, [the patient] drew a car”. Previously, the child would not draw anything but insects. He was also playing with other toys, besides bugs. The rhinitis had completely cleared on its own by this point. The child had a mild form of influenza. He had been less interested in dancing, and he was also sitting for longer periods in class. He would sit quietly “until he sees a bug”, at which point he would get up from his seat and chase it so that he may catch it. After the acute had passed, the child’s behaviour was still an issue |
Tarentula 201C was repeated |
| After 5 weeks | The mother had given the remedy in the morning and there was immediate mental and emotional improvement that very day, continuing into the following day.
His eye contact was good, he was engaging, and he was very settled. The mother was very happy with how the child had been sitting still in class. The teachers were also very happy. (During this time, the mother received results from a recent allergy test, which confirmed allergies to dairy, wheat, dust mites, cashews and almonds. The patient does not consume neither dairy nor wheat as the mother had already suspected this to be an allergen. However, the patient does enjoy almonds and cashews and would regularly be exposed to dust mites, particularly at school. Heightened histamine levels could be one possible explanation for his extreme behaviour). |
Wait |
| After 1 year and 6 months | The child and his mother had moved overseas during this time and therefore no follow ups were done earlier. No more Tarentula had been given; however, Ledum had been given recently for tick bites.
The “stretchy legs” has been completely gone for 6 months. The patient is still hot blooded. His sleep is still better (not disturbed) and he consistently sleeps in until 6/6:15am. He doesn’t get a sore belly anymore, still craves fat like avocado and salt, and he eats more cooked food than before. The child has had less intestinal worms, less often. He hasn’t been as sick – “he used to be sick every 3 weeks and now it’s once or twice a year”. Although he was mentally and emotionally much better overall, the child had begun to experience some difficulty with separation again. He also complained when things were “too noisy” and still had issues with his foreskin. He had begun “stimming” with his hands. The mother described it like a tick, where he gives a “thumbs up every 2 seconds” – he has been doing it to objects. His thumbs are hyper mobile and can bend backwards. He has been holding/scrunching his penis much less. He is always wriggling, fidgeting, and not relaxed. He doesn’t care about human feelings, just animals, insects, plants, and objects. He has been drawing a lot, is less interested in music, not dancing anymore, not hitting himself in the head, and is less obsessed about bugs; though, he now obsessed with plants. He still does not give much eye contact. |
Tarentula 1M |
| After 2 months | The child began vomiting, and 5 days after the remedy he had copious diarrheic stools. The mother described it as a “clearing out”. These gastrointestinal symptoms passed of their own accord quite quickly.
The thumb-flicking has almost gone completely. He was also less emotional, and seems to have become more emotionally resilient. The mother gave the following example of his plant being knocked over: She had thought to herself “I have to pick that up or he’ll be upset”; but then she forgot to do it. When the child saw the plant, he just picked it up and didn’t say anything. Normally, he would have carried on and cried about it. At school he now has his books on his desk – he sits and reads instead of leaving the classroom. |
Wait |
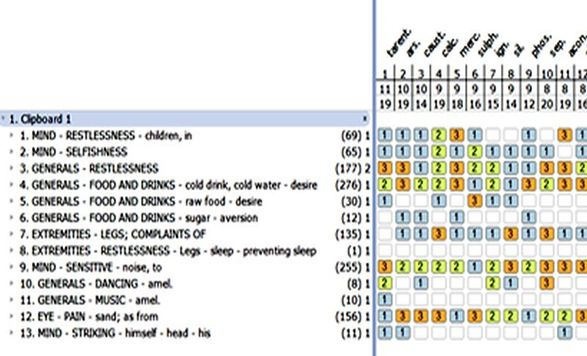
Repertorization 2.
Discussion
The remedy had to be repeated, and the child responded well to repeated dosing. However, it may have been better to increase the potency to a Tarentula 1M earlier. At the point where the hay fever symptoms had not progressed, the organism likely needed more of a push, and more of a physical reaction.
However, due to the child’s sensitive nature, a high potency was not given, despite the remedy picture being clear. Perhaps this approach contributed to a slower pace of healing. Having a long period between follow ups was not ideal, and the patient could have improved faster had there been earlier intervention. Yet, very important changes in the case remained resolved, such as improved sleep and the chief complaint of the restless “stretchy” legs.
Despite a few setbacks, the patient was consistently improving with sparse dosing of Tarentula 200C, and with this remedy the patient moved up to Level 4 Group B. As the case progressed, the tendency towards obsession remained, moving from insects and music to plants until it settled as a symptom overall, and the restlessness moved from the whole leg to just the hands and is now almost completely gone.
He no longer suffered infections of the urinary or reproductive spheres, which are lower forms of infection. After Tarentula 1M, a great physical reaction focussing on the gastrointestinal sphere was observed. It seemed that the susceptibility towards acute disease shifted from the lower respiratory system to the upper respiratory system then onto an even more superficial sphere, highlighted by a brief and less severe illness.
Since increasing the potency of the selected remedy, the patient’s Level of Health increased to Level 3 in Group A. His previous diagnosis of periodic limb movement disorder was no longer current, and the extreme restlessness of both the limbs and the mind that saw him wake a substantial 16 times an hour and to be physically held by his teachers to stop his movement, had been replaced by stability and calmness.
Conclusion
This case study also showcases the concept of the simillimum, and how one remedy can resonate powerfully and act for an extended period. It highlights how homeopathic treatment is more than just giving remedies for disorders; it is about tailoring the treatment towards the individual and monitoring a case and all its nuances.
Understanding the hierarchy within the three levels of the human being is paramount to monitoring the direction of cure and the positive progression of a chronic case. By treating the whole child, we saw a pleasant amelioration of the chief complaints, and improvements on the mental, emotional as well as physical levels.
REFERENCES
- Chabanov D, Tsintzas D, Vithoulkas G. Levels of Health Theory With the Example of a Case of Juvenile Rheumatoid Arthritis. J Evidence-based Integr Med. 2018;23. doi:10.1177/2515690X18777995
- A Case of Benign Rolandic Epilepsy Cured with Classical Homeopathy – Andrew Ward. Accessed August 30, 2021. https://hpathy.com/clinical-cases/a-case-of-benign-rolandic-epilepsy-cured-with-classical-homeopathy/
- Multiple Tics In A Boy To Be Enrolled In School – Kirsten Hill. Accessed August 30, 2021. https://hpathy.com/clinical-cases/multiple-tics-in-a-boy-to-be-enrolled-in-school/
- A S, J F, P R, E G, A B. Management of Self-injurious Behaviors in Children with Neurodevelopmental Disorders: A Pharmacotherapy Overview. Pharmacotherapy. 2019;39(6):645-664. doi:10.1002/PHAR.2238
- Vithoulkas G. Levels of Health.; 2017.